Lesion Characteristics
Lesion Size (diameter): 8 mm
Lesion Location: Right upper lobe (RUL) lesion
Bronchus Sign: No
Visible on Fluoro: No
REBUS Verification: Yes
Case Information
Full Procedure Time: 50 minutes
ROSE: Atypical
Final Pathology Report: Adenocarcinoma
Patient Background
A 62 year-old patient with stage 4 lung cancer and cancer history. In 2017, the patient had a craniectomy for an oligometastatic cranial metastasis and definitive chemoradiation for left lobe lung cancer. A recent CT scan showed a new, 8 x 9 mm right upper lobe (RUL) nodule with mild uptake on PET.
An Ethicon MONARCH™ robot-assisted bronchoscopy procedure with LungVision™ intraoperative CT imaging and r-EBUS was scheduled.
The Procedure
Planning
During planning, a preoperative CT is loaded onto the LungVision™ system and the lesion is marked and contoured so that the LungVision™ AI-driven intraoperative CT imaging system has an approximation of the lesion size, shape and location prior to beginning the procedure. The LungVision™ software derives the airways from the preoperative CT and for those who are looking to use LungVision™ as a standalone, navigation bronchoscopy system, a virtual bronchoscopy highlighting the preferred pathway with turn-by-turn guidance to the lesion is provided. In this case, an Ethicon MONARCH™ robot was used to navigate to the lesion.
Registration
Registration of the LungVision™ system consists of two C-arm spins – one around the main carina and another iso-centered around the lesion. These two spins, completed with Crozer’s GE OEC 9900 Elite C-arm produce an initial intraoperative CT scan that shows the actual lesion and lesion location prior to navigation.

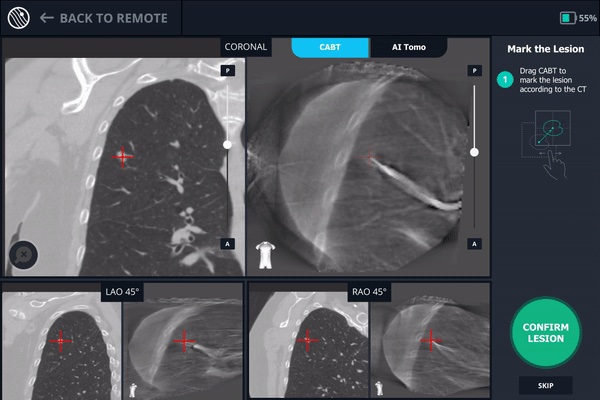
Main carina marking on Body Vision’s C-Arm Based Tomography (CABT) during registration.

Lesion marking on Body Vision’s CABT during registration.
Registration of the Body Vision system is complete and registration of the MONARCH robot is performed.
Navigation
The MONARCH robot was used to navigate out to the virtual target. Once at the target location as defined by MONARCH a radial endobronchial ultrasound (r-EBUS) probe was inserted down the working channel of the MONARCH to confirm the lesion location. No r-EBUS signal was returned initially so Body Vision’s augmented fluoroscopy was used to guide realignment of the bronchoscope.


Realignment of the bronchoscope as visualized under Body Vision’s augmented fluoroscopy.
Tool-in-Lesion Confirmation
After realigning the bronchoscope, another C-arm spin was performed to create an updated LungVision™ CABT scan to ascertain the new lesion-tool relationship. This new CABT scan provided visual confirmation that after realignment of the bronchoscope, tool-in-lesion was achieved.

Body Vision’s C-arm based tomography (CABT) scan providing visual confirmation of tool-in-lesion after bronchoscope realignment.
Following tool-in-lesion confirmation with LungVision™, a radial endobronchial ultrasound (r-EBUS) probe was inserted down the working channel of the MONARCH to provide a secondary confirmation of lesion location.
Biopsy
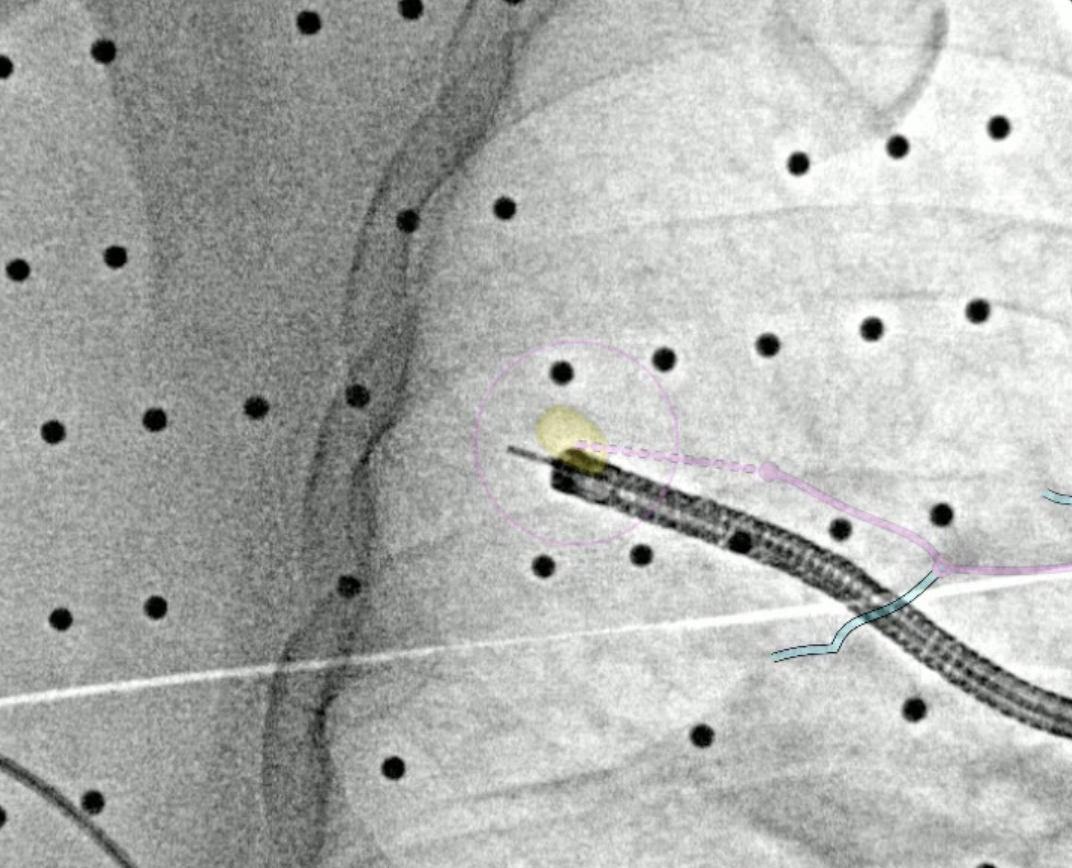
After the r-EBUS probe returned a positive signal, biopsy samples via biopsy needle and forceps were acquired under Body Vision’s real-time, augmented fluoroscopy to ensure that the samples were taken from within the lesion. A fiducial marker was also placed using Body Vision’s augmented fluoroscopy for visual guidance. Rapid On-Site Evaluation (ROSE) confirmed that the tissue samples were atypical and the final pathology report stated adenocarcinoma.

Tissue samples acquired via biopsy needle as seen under Body Vision’s augmented fluoroscopy.

Tissue samples were also acquired via forceps as seen under Body Vision’s augmented fluoroscopy.

A fiducial marker being placed using Body Vision’s augmented fluoroscopy for guidance.
Final Pathology
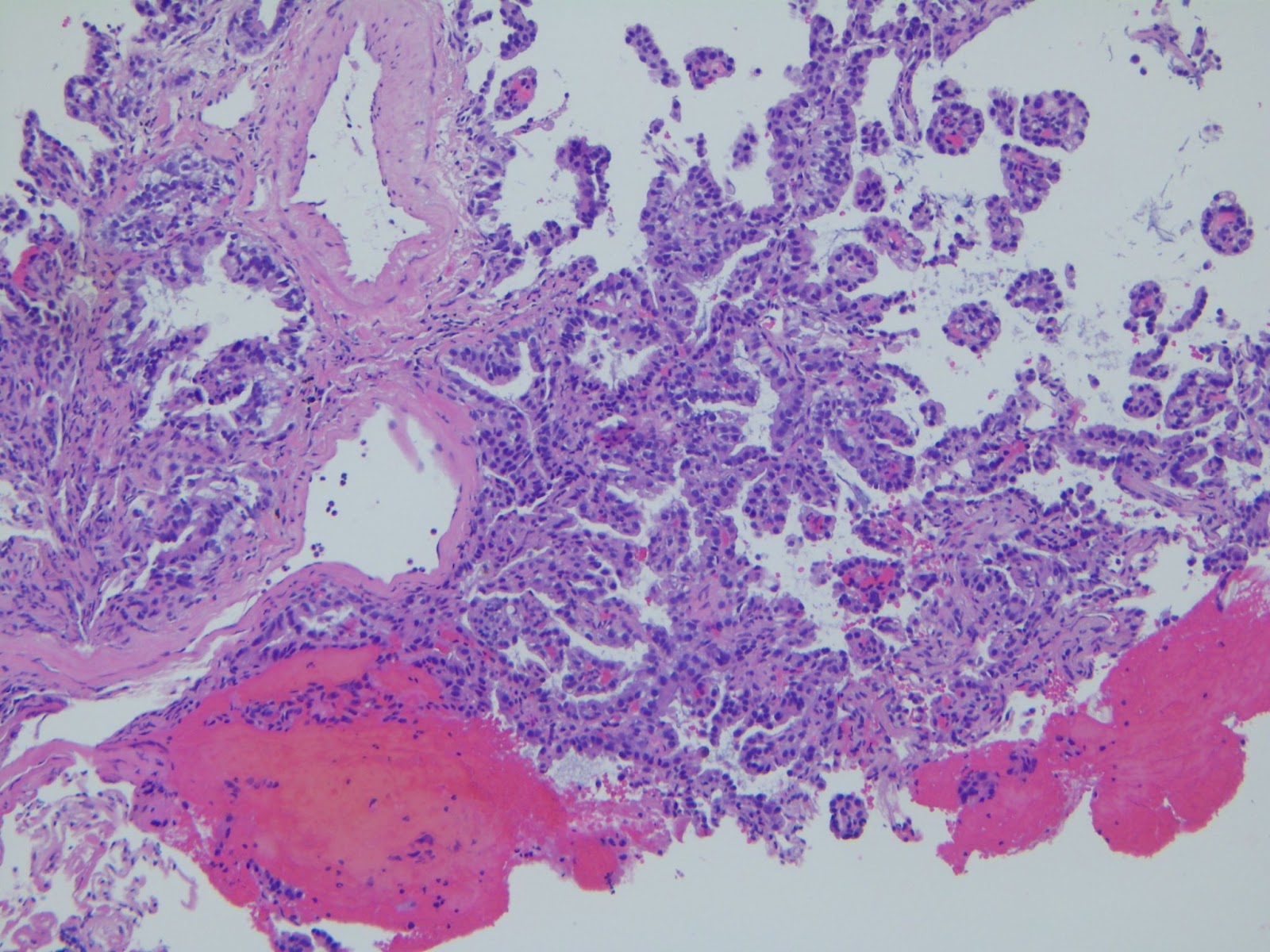
The final pathology report confirmed adenocarcinoma.
Conclusion
This case demonstrates how the LungVision™ system seamlessly integrates with and enhances the Ethicon MONARCH robotic bronchoscope with real-time, intraoperative CT imaging functionality that proved critical for overcoming CT-to-body divergence and tool-in-lesion confirmation prior to biopsy. For this patient, LungVision™ enabled the biopsy, definitive diagnosis of and fiducial marker placement within this small, subcentimeter lesion.
About Dr. Whitlark

Joseph D. Whitlark, MD
Robotic Thoracic Surgeon
Crozer Health