Lesion Characteristics
Lesion Size (diameter): 7mm
Lesion Location: Right Lower Lobe (RLL), medial basal, middle 1/3
Visible on Fluoro: No
REBUS Verification: No
Case Information
Full Procedure Time: 30 Minutes
ROSE: Non-diagnostic, blood
Final Pathology Report: Metastatic Thyroid Cancer
Patient Background
An 81-year-old female and former 40-50 pack-per-year smoker with a prior cancer history of the breast, thyroid, and pancreas presented with the symptom of a productive cough. A diagnostic bronchoscopy was scheduled to acquire tissue samples from the lesion to determine the best course of treatment.
The Procedure
Planning
During planning on the LungVision™ system, a preoperative CT is loaded and the lesion is marked and contoured so that the system has an approximation of the lesion size, shape and location prior to beginning the procedure. The LungVision™ system also derives the airways from the preoperative CT, and for those looking for a complete navigation bronchoscopy system, a virtual bronchoscopy highlighting the preferred pathway to the lesion can be provided. In this case, an Ethicon MONARCH™ robotic bronchoscopy platform was used to navigate out to the lesion.
Registration
Once the patient is on the table, LungVision™ registration consists of two C-arm spins – one iso-centered around the main carina and another around the lesion. These spins produce an initial C-Arm Based Computed Tomography (CABT) scan confirming actual lesion and lesion location prior to navigation.
Marking the main carina on LungVision’s CABT during registration.
Lesion marking on LungVision’s AI Tomography during registration.
Navigation
Navigation to the lesion was performed using Ethicon MONARCH™ robot’s electromagnetic navigation (EMN) system. LungVison’s augmented fluoroscopy provided real-time imaging of the bronchoscope and lesion location during navigation.

LungVision™ augmented fluoroscopy during navigation.
Tool-in-Lesion Confirmation
Once at the target lesion location as defined by the Ethicon MONARCH™ robot, a biopsy needle was introduced down the working channel of the bronchoscope and another C-arm spin was performed to confirm tool-in-lesion in multiple 3D planes using LungVision’s intraoperative CT imaging.
LungVision™ C-Arm Based Tomography (CABT) imaging showing tool-in-lesion confirmation.
LungVision™ AI Tomography imaging showing tool-in-lesion confirmation.
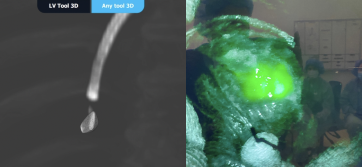
LungVision providing an interactive 3D View of the intraoperative CT scans showing tool-in-lesion confirmation.
Biopsy and Dye Marking for Resection
Following tool-in-lesion confirmation, samples were acquired first via biopsy needle and then via biopsy forceps under LungVision’s real-time, augmented fluoroscopy. Rapid On-Site Evaluation (ROSE) returned a non-diagnostic ROSE call of blood during the procedure.

Needle biopsy performed under LungVision’s real-time, augmented fluoroscopy.
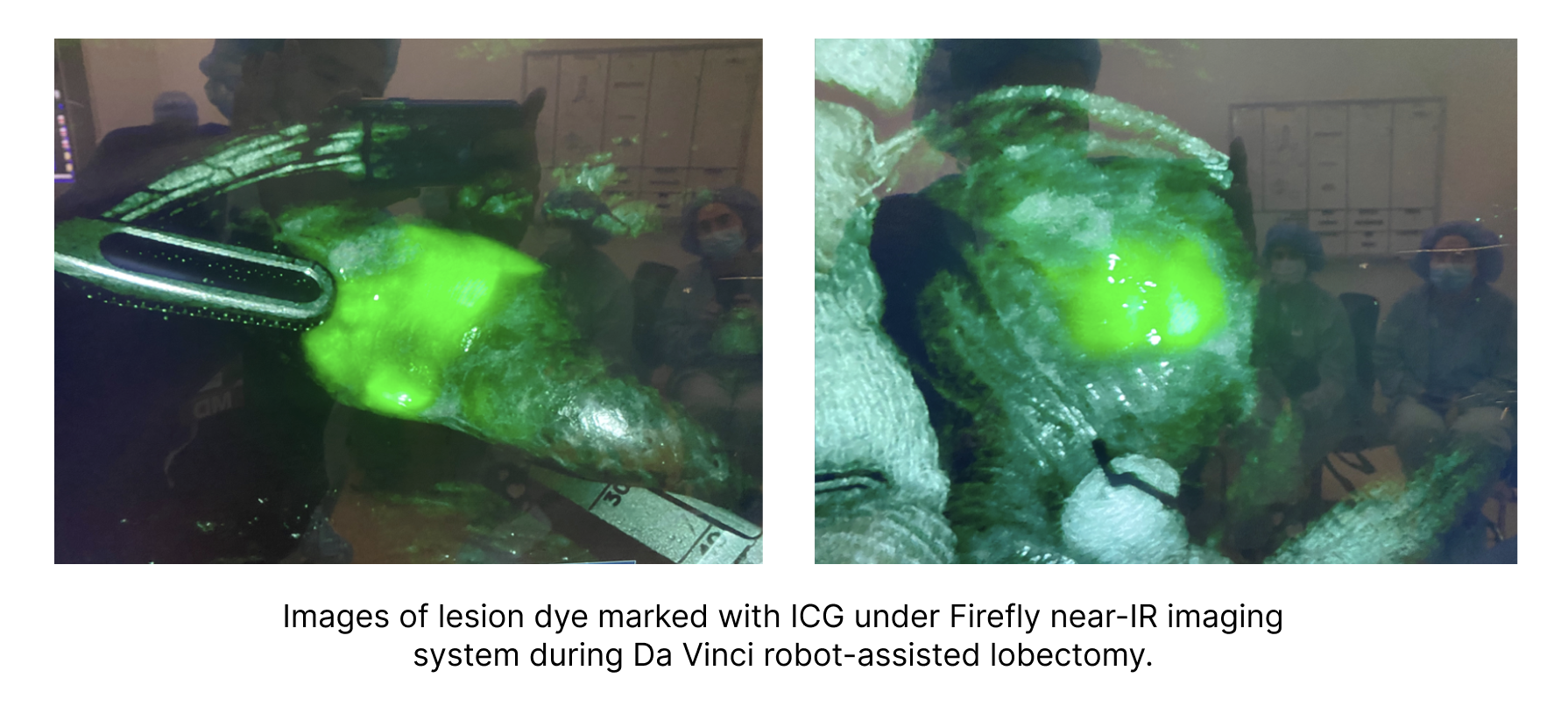
Although ROSE did not come back with a definitive call for cancer, there was enough indication of cancer based on patient history and symptoms that the physician decided to proceed with dye marking and wedge resection for a definitive diagnosis. Under LungVision’s real-time augmented fluoroscopy, fiducial coils dipped in indocyanine green (ICG) were placed into the lesion to dye mark the lesion for a subsequent robot-assisted wedge resection with Firefly™ near-IR imaging in order to visualize the ICG.
Placement of fiducials dipped in ICG to dye mark lesion for subsequent wedge resection.
Final Pathology
The wedge resection was sent to pathology and the final pathology report stated metastatic thyroid cancer.
Conclusion
LungVision's intraoperative CT imaging provided confirmation of tool-in-lesion and real-time imaging of the lesion to enable the accurate dye marking needed for a precise wedge resection of the suspicious pulmonary lesion for both diagnosis and treatment in a single-anesthesia event.
About Dr. Tsai

Wilson Tsai, MD
Director, Thoracic Program
John Muir Health